Elderly female with a history of hypertension, stroke, and, 1 month before, heart attack with cardiac arrest. The patient presented to the emergency department with 1 day of nausea, vomiting, cold sweats, and malaise. Troponins 1.54. ECG with inferior Q waves but no ST elevation/depression or T-wave inversion.
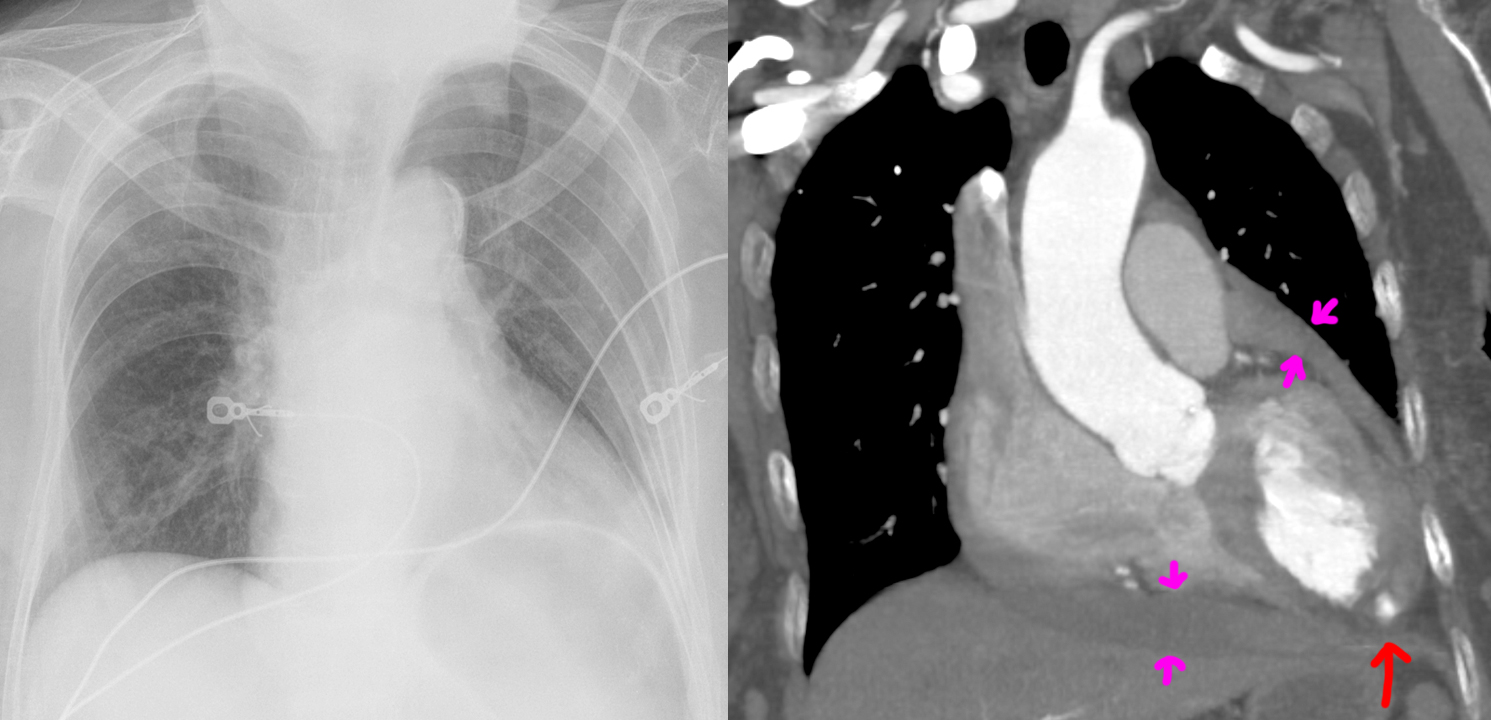
Chest radiograph shows an enlarged cardiac silhouette, for which a differential of cardiomegaly or pericardial effusion was suggested, as well as increased pulmonary vascular markings compatible with pulmonary congestion. Compared chest radiograph findings to the images from the methamphetamine-induced cardiomyopathy case.
CT angiography shows both cardiomegaly as well as an intermediate-density pericardial effusion (magenta arrows) concerning for hemopericardium. Most concerningly (holy-shit concerningly), there is a left ventricular aneurysm with rupture and blush of contrast (red arrow) into the hemopericardium, compatible with ongoing bleeding.
It is not surprising that a rupture of the heart carries high mortality risk. The patient passed away from PEA cardiac arrest shortly after admission, likely from cardiac tamponade by the enlarging hemopericardium.